Non- Cardiac Chest Pain
OVERVIEW | CAUSES | RISK FACTORS | SYMPTOMS | COMPLICATION | DIAGNOSIS | TREATMENT | PREVENTION | REFERENCES
OVERVIEW
Non-cardiac chest pain is the term that is used to describe pain in the chest that is not caused by heart disease or a heart attack.
Non-cardiac chest pain is often described as feeling like angina, the chest pain caused by heart disease. The patient feels a pressure or squeezing pain behind the breast bone. Some people also report the pain spreads to the neck, left arm, or back. The pain can last for a few minutes or for hours.
CAUSES
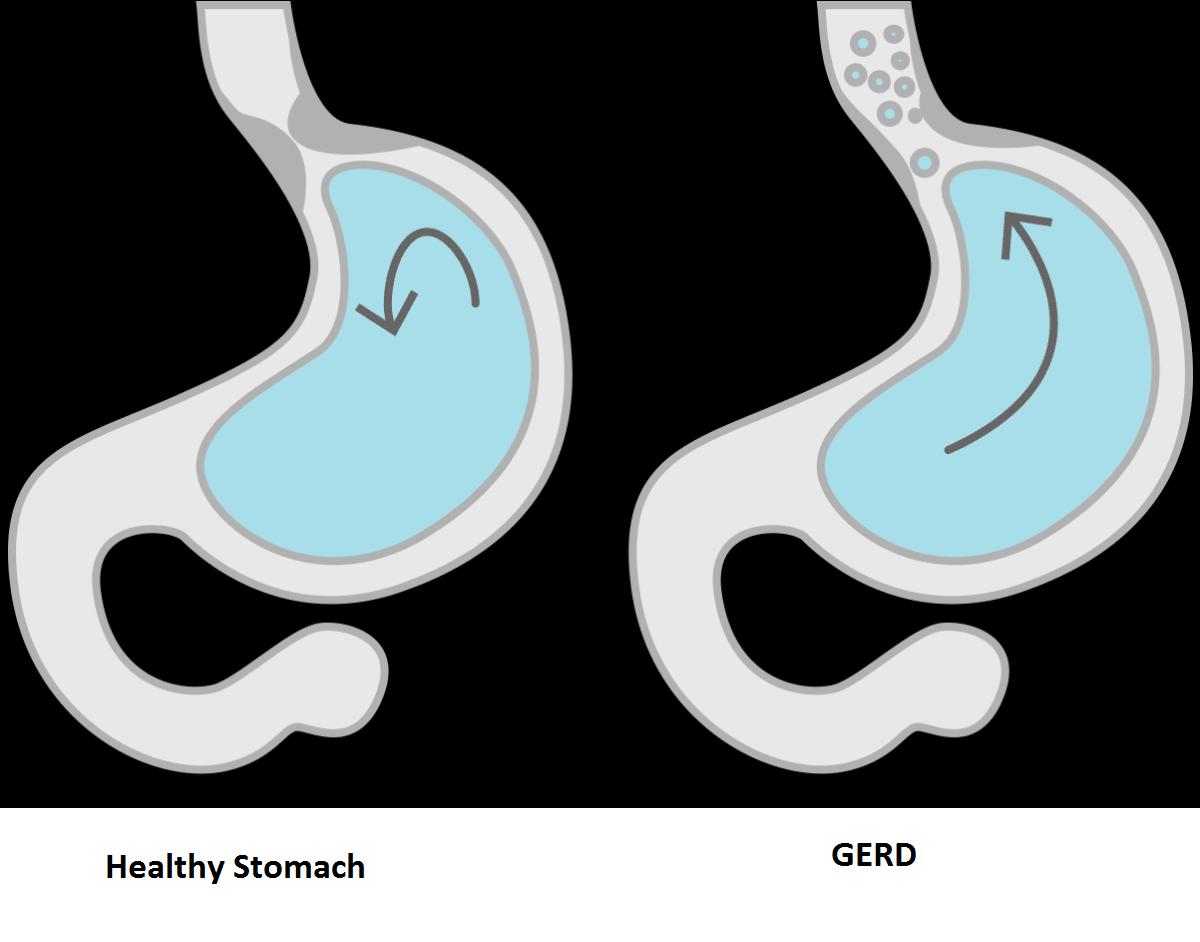
In most people, non-cardiac chest is related to a problem with the esophagus, the tube that connects the mouth with the stomach. There are several different esophagus problems that can cause non-cardiac chest pain.
Gastroesophageal reflux disease (GERD) is the most common cause of non-cardiac chest pain. Also called acid reflux, this condition causes 22 to 66 percent of non-cardiac chest pain.
Other, less common esophagus problems that can cause chest pain include:
- Muscle problems, also called esophageal motility disorders. In people with these problems, abnormal muscle activity in the esophagus prevents food from moving through the esophagus normally. Esophagus muscle problems include uncoordinated muscle contractions (esophageal spasm), high-pressure contractions or squeezing of the esophagus (nutcracker esophagus), and missing contractions caused by nerve loss (achalasia).
- Visceral or esophageal hypersensitivity. People with this condition have a lot of pain when there is a very small pressure change in the esophagus or a small amount of stomach acid comes up into the esophagus. People with a normal esophagus would not feel anything from the pressure change or the presence of acid. The reason why some people have this extra sensitivity (hypersensitivity) to pressure or acid is not known.
What other problems can cause non-cardiac chest pain?
Some less-common problems that can cause non-cardiac chest pain include:
- Muscle or bone problems in the chest, chest wall, or spine (back)
- Lung conditions or diseases, including diseases of the pleura, the tissue that covers the lungs
- Stomach problems, such as ulcers
- Stress, anxiety, or depression.
RISK FACTORS
NCCP can occur in children as well as older patients, it also affects men and women and some studies have suggested a higher proportion of patients are female. The reasons some studies have found women may have a higher frequency of NCCP than men is not well understood.
SYMPTOMS
Non Cardiac chest pain typically is felt behind the breast bone (sternum) and is described as oppressive, squeezing or pressure-like. It may radiate to the neck, left arm or the back (the spine). It may be precipitated by food intake. It lasts variable periods of time and it is not unusual for it to last hours.
Patients may also complain of associated reflux symptoms such as heartburn (a burning feeling behind the breast bone) or fluid regurgitation (a sensation of stomach juices coming back toward the chest and even to the mouth frequently with a bitter or sour taste).
COMPLICATIONS
A person should receive immediate medical attention for chest pain, even if the cause does not turn out to be a heart condition.
It is especially important to receive urgent care if any of the following accompany chest pain:
- Confusion
- Dizziness
- Nausea
- Shortness of breath
- Weakness
- Numbness
If a person recognizes the cause of their chest pain, such as acid reflux or COPD, they should contact their doctor if the symptoms worsen.
While non-cardiac chest pain rarely indicates a serious health condition, it is best to get your health diagnosed.
DIAGNOSIS
The person having chest pain cannot know whether it is heart related or is non-cardiac chest pain. A person having unexplained chest pain should go to the emergency room.
The emergency room doctor first will give the patient a complete physical exam that includes temperature, blood pressure, and heart rate. Next the doctor will test the patient for heart disease or heart attack. These tests include an electrocardiogram (a noninvasive test that records the heart’s electrical activity) and blood tests. The heart releases certain proteins when a heart attack occurs that will show up in a blood test.
If these tests show that the heart is fine and the pain is not from a heart attack, the pain is called non-cardiac chest pain.
TREATMENT
Patients may be treated as if the NCCP was a result of having GERD:
Once cardiac and other life-threatening conditions have been excluded and, based on the notion that the most common cause of NCCP is GERD, a treatment trial is frequently considered.
Patients are often prescribed a proton pump inhibitor (PPI) also called a PPI trial. They must be taken at least 30-60 minutes before breakfast. It has been shown that this approach produces an approximately 80% response rate for patients with GERD-related NCCP. (source)
If the patient responds, the treatment can be continued for at least 8 weeks at a reduced dose such as Omeprazole (or equivalent PPI medication ) 20 mg twice daily about 40 min prior to meals. Other equivalent PPI’s can also be employed and include: Esomeprazole, Lansoprazole, Rabeprazole, and Pantoprazole.
For patients not responding to a PPI, GERD is the unlikely source of pain:
For these patients, other medications are available. These medications are felt to produce their favorable effect by reducing pain transmission from the esophagus to the brain. The medications often used are low doses and are from the class of drugs known as tricyclic antidepressants (TCAs), and not used at the high doses employed for the treatment of depression.
Commonly used agents are amitriptyline, nortriptyline, desipramine, imipramine and trazodone. The two most commonly used agents are imipramine and trazodone. While for the most part they are safe, side effects may include sleepiness, dry mouth, blurred vision and urinary retention. Trazodone can also cause a sustained erection (called priapism), which is considered a medical emergency.
Other categories of antidepressants – such as “selective serotonin reuptake inhibitors” or SSRI” – can be tried if TCA are not tolerated because of side effects. Two recent reports suggest that the SSRI Sertraline may also have a beneficial effect in the treatment of NCCP. This medicine was found to be more effective than placebo (a sugar pill or an inert substance) in the treatment of NCCP. New studies are also being done to explore other SSRI’s like paroxetin, fluoxetin and citalopram. Also recent studies have found potential benefit with the Serotonin and Noradrenalin Reuptake Inhibitor (SNRI) called Venlafaxine. For patients not responding to either acid inhibition trial or TCA or other antidepressants, esophageal motility testing (a study done to evaluate the muscle contractions of the swallowing pipe) may be done to look for other uncommon causes of chest pain such as achalasia. This is particularly important since achalasia is a treatable disorder.
A number of studies continue to be done to better understand the mechanism(s) of pain in NCCP. Furthermore, new treatment agents are being investigated. A recent study suggested that receptors in the esophagus, such as the so called adenosine receptors, may account for visceral pain in NCCP. Using a medication that acts on these receptors (Theophilline) a group of investigators showed it may be effective for the treatment of NCCP. However, side effects of this particular agent may limit its use. Thus, in the future newer medications that act on these adenosine receptors but that have a better margin of safety may provide new opportunities for the treatment of this challenging condition.
Management of stress:
If patients do not respond to the above approach or they suffer from depression, anxiety, and/or panic disorder, they should be referred for appropriate psychiatric consultation and treatment. Several recent studies have also found that Cognitive Behavioral Therapy (CBT) or “talk therapy” and relaxation training techniques is effective in improving NCCP when compared to patients on a waiting list. Other brief preliminary reports have also found that hypnosis may also help selected patients with NCCP.
Most non-cardiac chest pain is caused by GERD. People who follow their doctor’s instructions for managing GERD usually do not have further problems with non-cardiac chest pain.
REFERENCE
- https://gi.org/topics/non-cardiac-chest-pain/
- https://my.clevelandclinic.org/health/diseases/15851-gerd-non-cardiac-chest-pain
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3093002/
- https://pubmed.ncbi.nlm.nih.gov/29642692/