Rectum Anatomy, Rectum Functions, Rectum Conditions, Rectum disorders
Rectum- Anatomy, Functions and Conditions
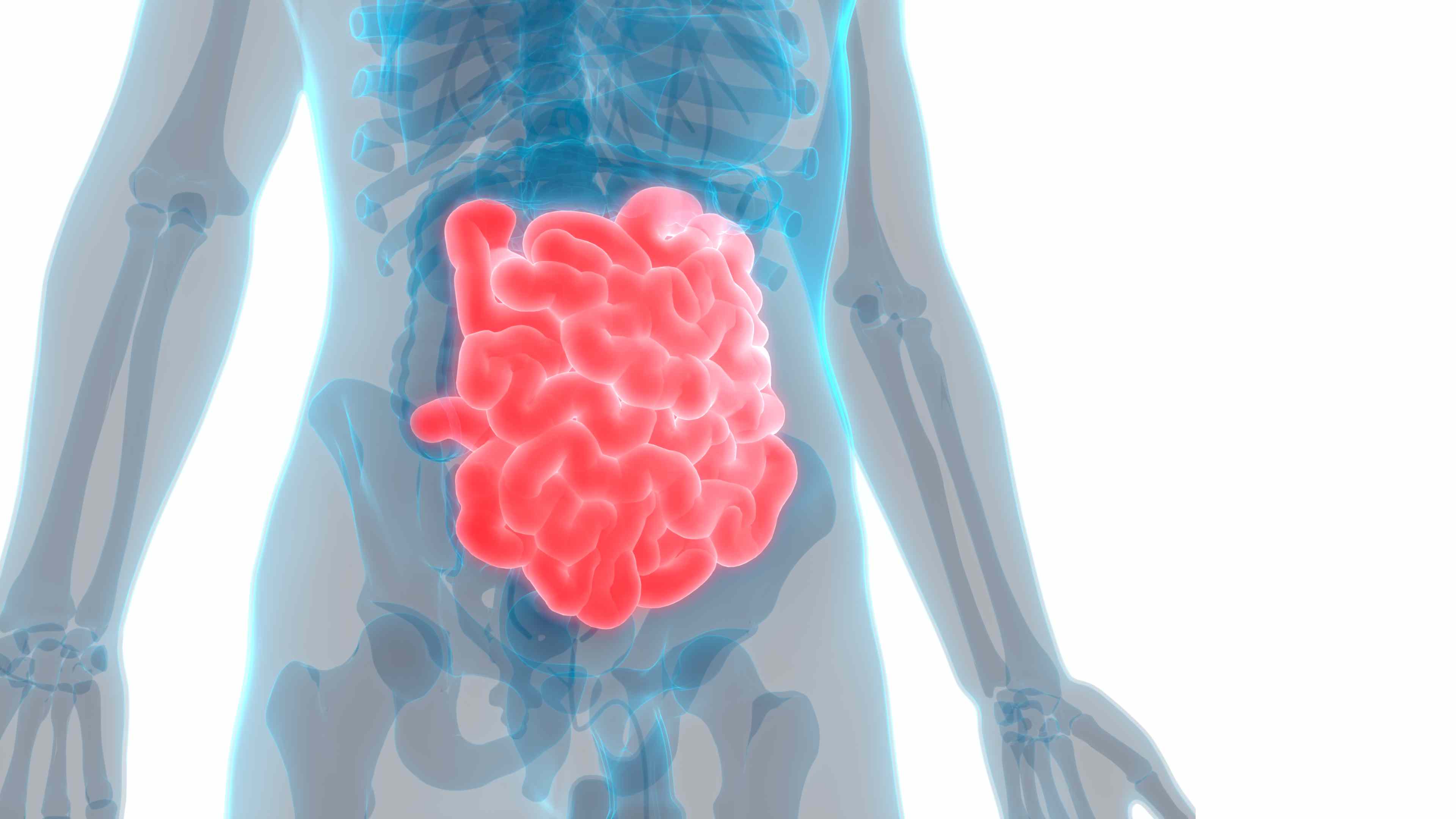
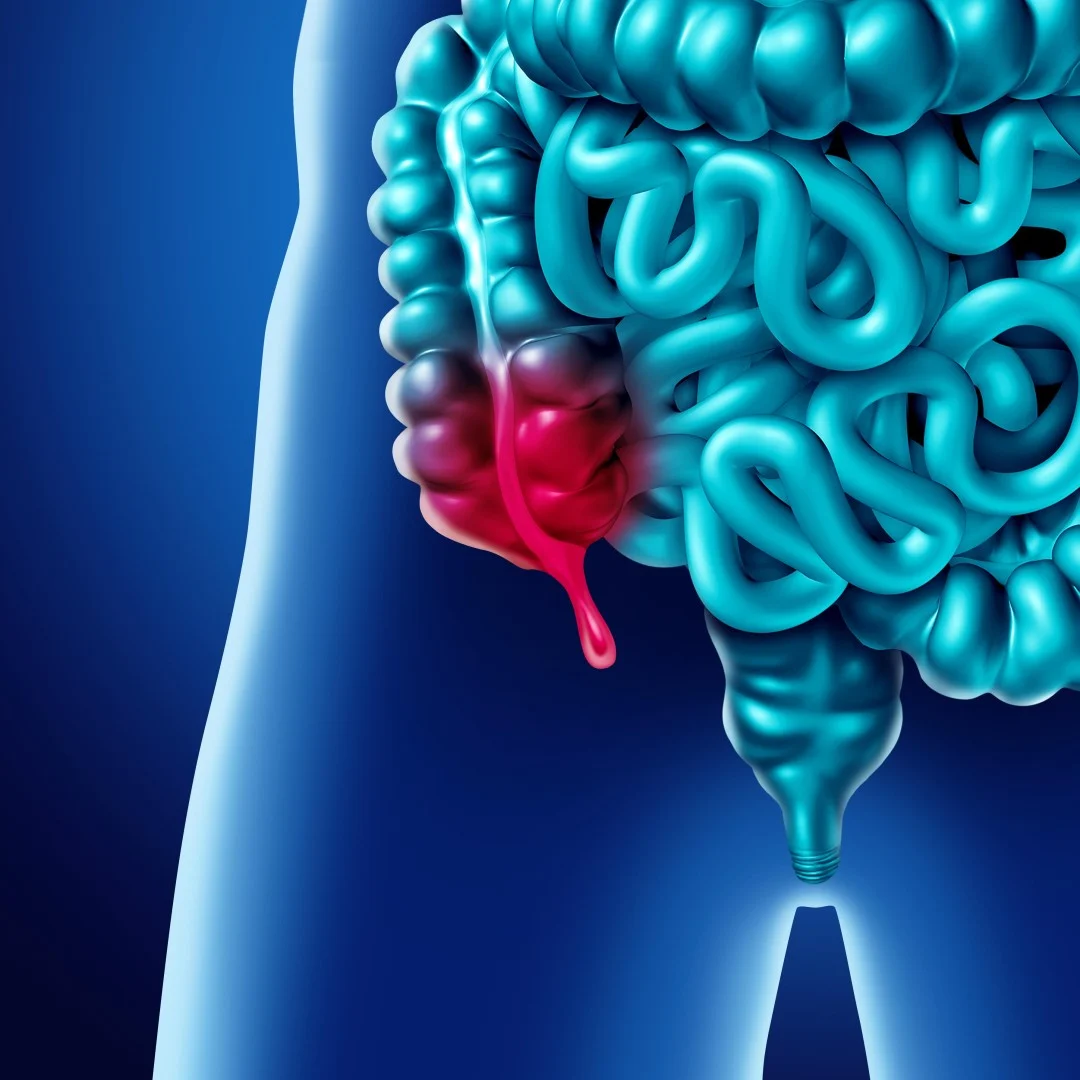
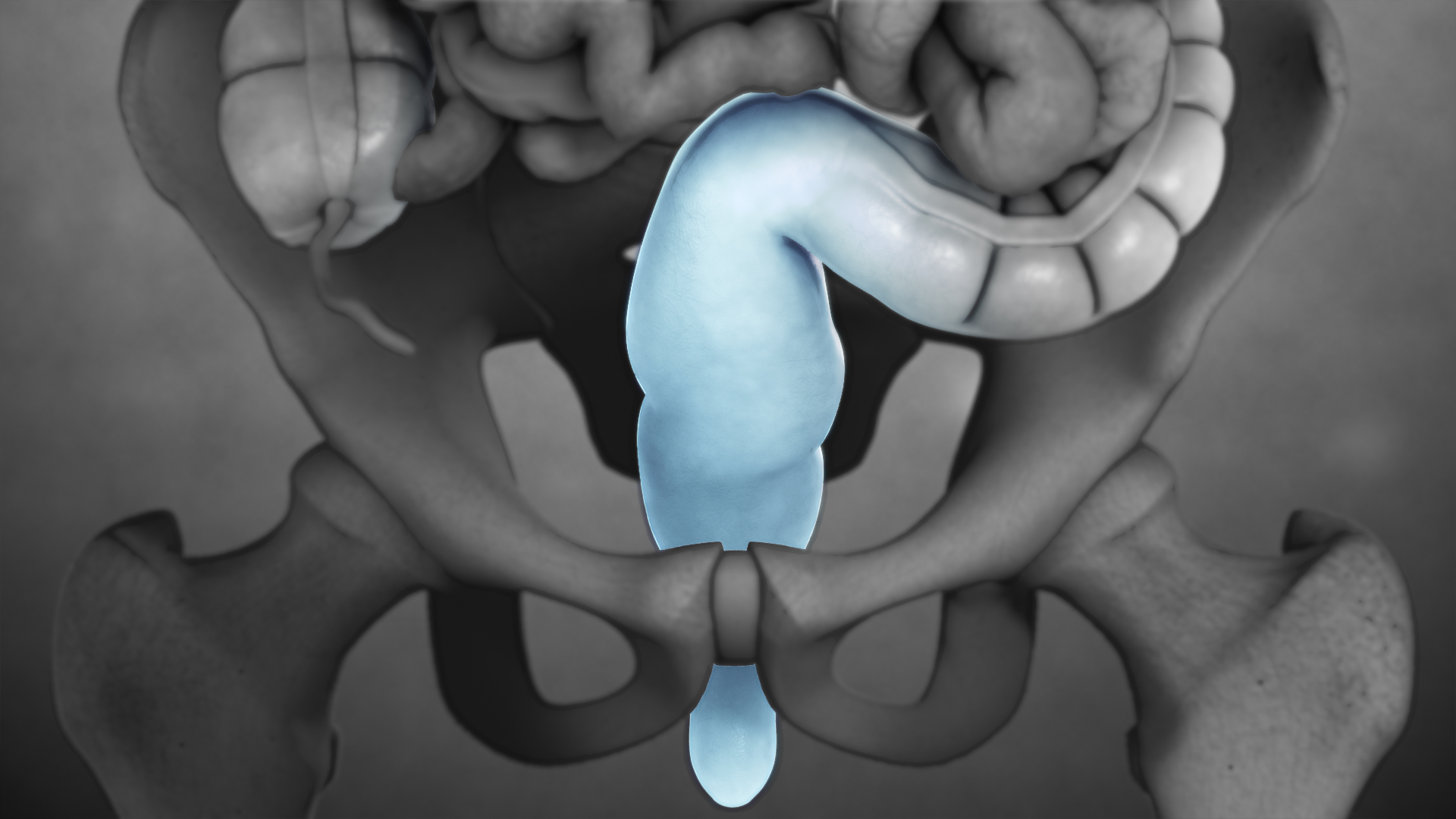
The rectum is the concluding part of the large intestine that terminates in the anus.
Rectum Overview
Rectum is the terminal segment of the digestive system in which feces accumulate just prior to discharge. The rectum is continuous with the sigmoid colon and extends 13 to 15 cm (5 to 6 inches) to the anus. A muscular sheet called the pelvic diaphragm runs perpendicular to the juncture of the rectum and anal canal and maintains a constriction between these two segments of the large intestine. The internal cavity of the rectum is divided into three or four chambers; each chamber is partly segmented from the others by permanent transverse folds (valves of Houston) that help to support the rectal contents. A sheath of longitudinal muscle surrounds the outside wall of the rectum, making it possible for the rectum to shorten in length.
Rectum Anatomy
Macroscopic anatomy
The rectum has two flexures: The sacral flexure (dorsal bend) results from the concave form of the sacrum, the perineal flexure (ventral bend) from the encirclement of the rectum by the levator ani muscle (puborectal sling). Here is the point of transition to the anal canal (anorectal junction).
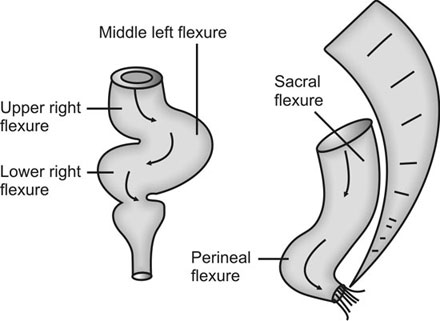
Morphologically the rectum is similar to the rest of the large intestine. However it does not have taeniae, haustra, appendices epiploicae and semilunar folds. Characteristic are the three constant transverse folds (Houston’s valves). The middle rectal fold (Kohlrausch’s valve) is the strongest and located about 7 cm from the anus. Tumors below this fold may be palpable during digital rectal examination. The rectal ampulla (section between Kohlrausch’s valve and anorectal junction) is quite stretchable and serves as a reservoir during defecation.
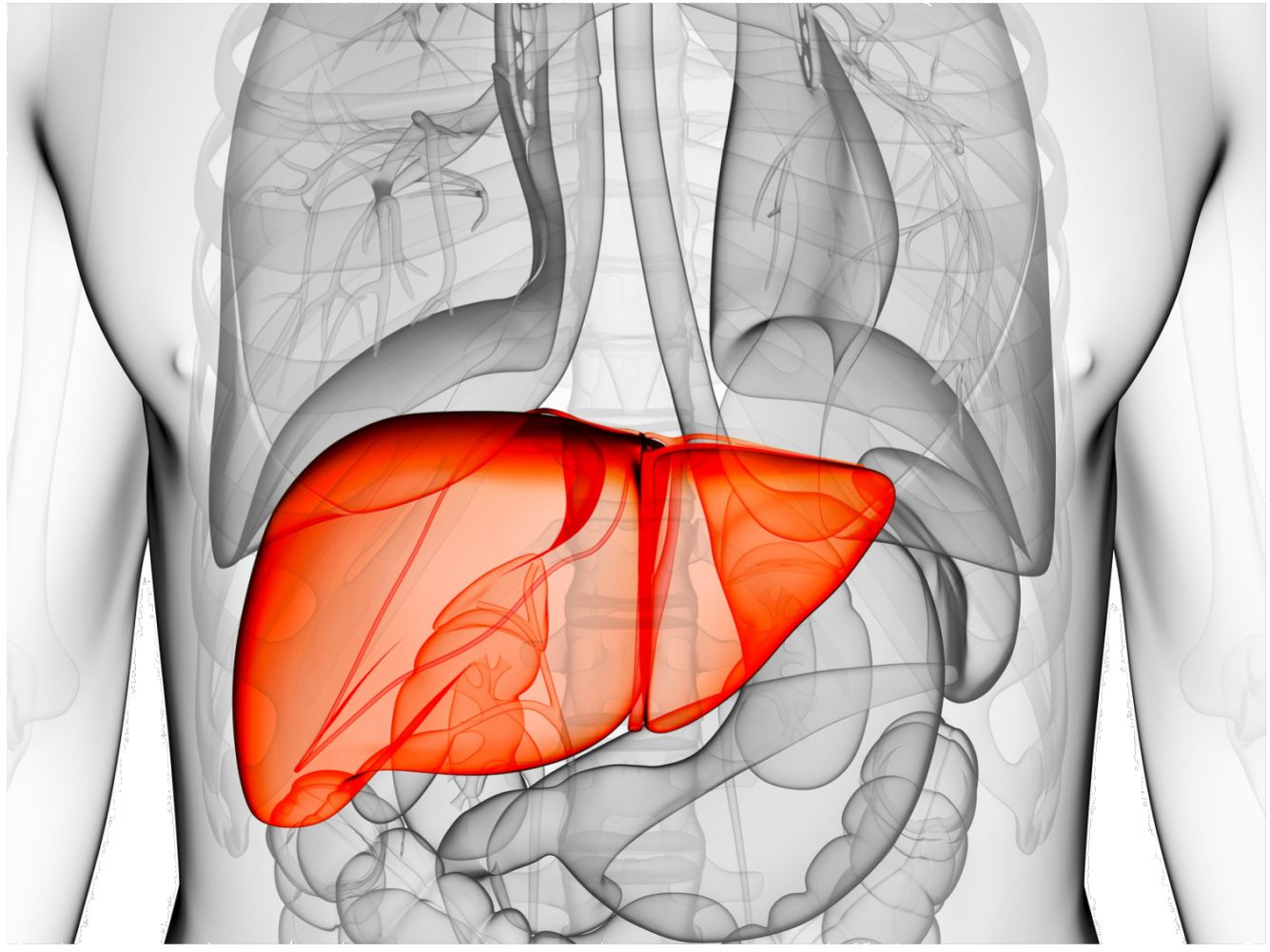
The rectum is supplied by the superior rectal artery (branch of the inferior mesenteric artery), middle rectal artery (branch of the internal iliac artery) and inferior rectal artery (branch of the internal pudendal artery from the internal iliac artery). The lymph vessels course along the veins which is why proximal rectal carcinoma metastasizes preferentially to the liver whereas distal rectal carcinoma rather metastasizes to the lungs. The sympathetic innervation is carried by the inferior mesenteric plexus, the parasympathetic innervation by the pelvic splanchnic nerves and the inferior hypogastric plexus.
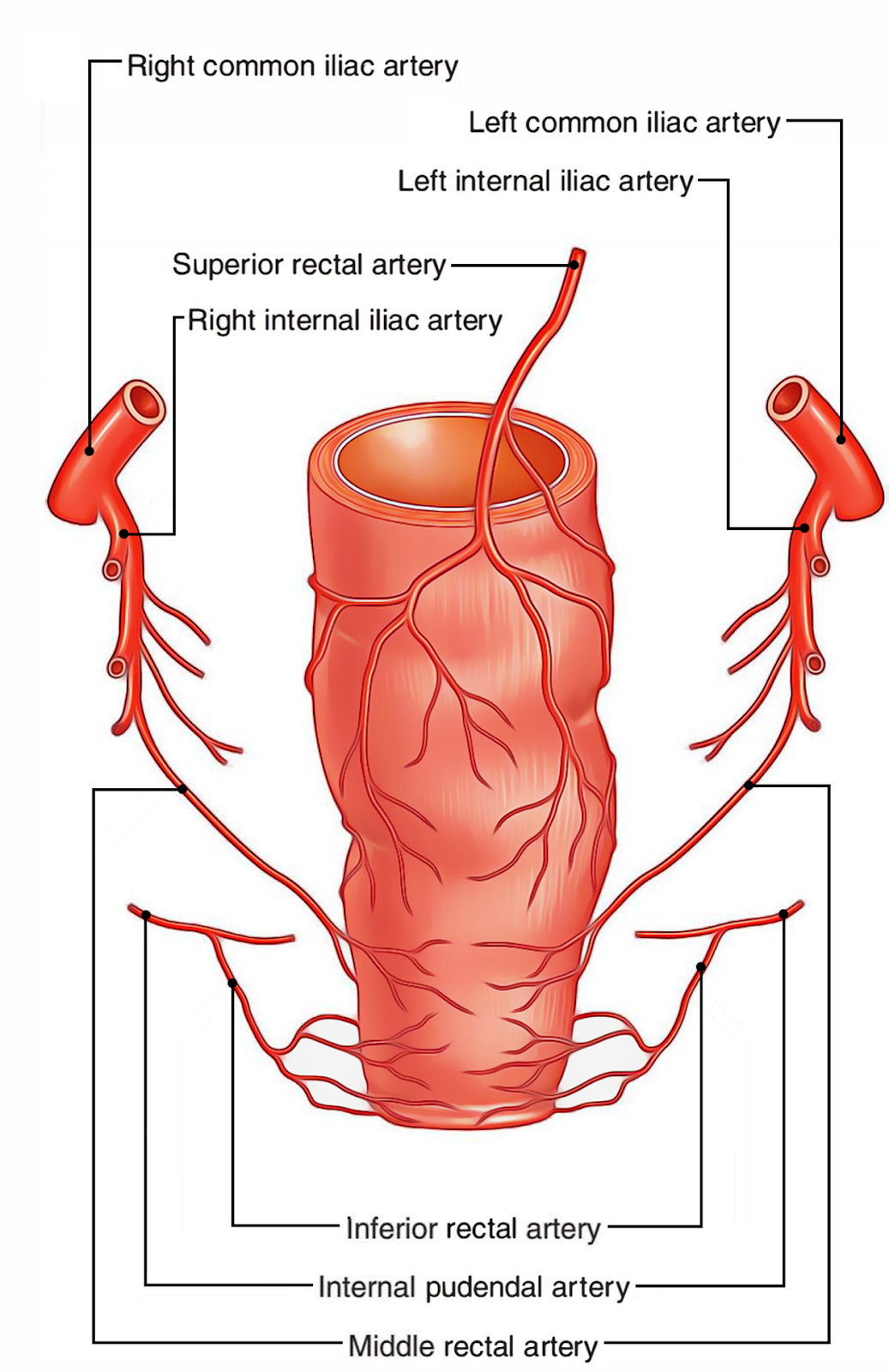
The venous drainage of the rectum is carried out by the superior, middle and inferior rectal veins. The superior rectal veins drain the upper part of the rectum into the portal venous system (through the inferior mesenteric vein); on the other hand, the middle and inferior rectal veins drain the lower part of the rectum into the internal iliac vein (systematic circulation) via the internal pudendal vein. Between those two different types of veins (the ones that drain to the hepatic portal system and the ones that drain systematic circulation) there are anastomoses which are clinically important in cases of portal hypertension.
Microscopic anatomy
Histologically the rectum is similar to the rest of the large intestine with its usual structure: mucosa, submucosa, muscularis and serosa/adventitia. You can easily remember these layers using the mnemonic 'M.S.M.S'.
- The mucosa has the typical intestinal epithelium with simple columnar enterocytes and numerous goblet cells. At the anal transitional zone the columnar epithelium flattens more and more and eventually becomes stratified squamous non-keratinized epithelium.
- The epithelial layer is followed by the connective tissue layer (lamina propria) with blood and lymph vessels and a muscle layer (lamina muscularis mucosae).
- The submucosa contains loose connective tissue with blood vessels, lymph follicles and the Meissner's plexus. It has a dense network of veins (rectal venous plexus) and is thickened at the transverse folds.
- The muscularis has the typical inner circular and outer longitudinal musculature between which the Auerbach’s plexus lies. The ring musculature continues as the sphincter ani externus muscle within the sphincter system whereas the outer longitudinal musculature continues as the corrugator cutis ani muscle inserting at the skin around the anus.
Rectum Function
The rectum is the last stop before the feces is eliminated through the anal canal. Similar to the colon electrolytes are absorbed (sodium, potassium, chloride) and indigestible food ingredients are decomposed by anaerobic bacteria. The stool is thickened through water absorption and mixed with mucus.
Furthermore the rectum is part of the continence organ and plays an important role in the mechanism of defecation. If stool enters the rectal ampulla which is usually empty it is registered by stretch receptors. The information is transferred to the central nervous system giving the person the urge to defecate. He can now decide to either initiate or delay the defecation by relaxing or tensing the levator ani muscle and sphincter ani externus muscle.
However the rising pressure in the ampulla leads to an increasing relaxation of the involuntary smooth corrugator cutis ani muscle and sphincter ani internus muscle (rectoanal inhibitory reflex) which is why holding in the stool for a long time involves an increasing “effort”. The rectum supports the defecation through contraction. Additionally the intra-abdominal pressure is increased through the voluntary tension of the diaphragm and abdominal muscles (abdominal press).
Rectum Disorder and related health conditions
The rectal lining consists of glistening red tissue containing mucus glands- much like the rest of the intestinal lining. The lining of the rectum is relatively insensitive to pain, but the nerves from the anus and nearby external skin are very sensitive to pain.
The veins from the rectum drain mostly into the portal vein, which leads to the liver, and then into the general circulation. Some of these veins drain directly into the pelvic veins and then into the general circulation. The lymph vessels of the rectum drain into lymph nodes in the lower abdomen.
Disorders of the rectum include
- Anorectal abscess
- Anorectal fistula
- Colorectal cancer
- Fecal incontinence
- Foreign objects in the rectum
- Hemorrhoids
- Levator syndrome
- Pilonidal disease
- Proctitis
- Rectal prolapse
- Rectal Bleeding
Rectum Diagnosis and Treatment
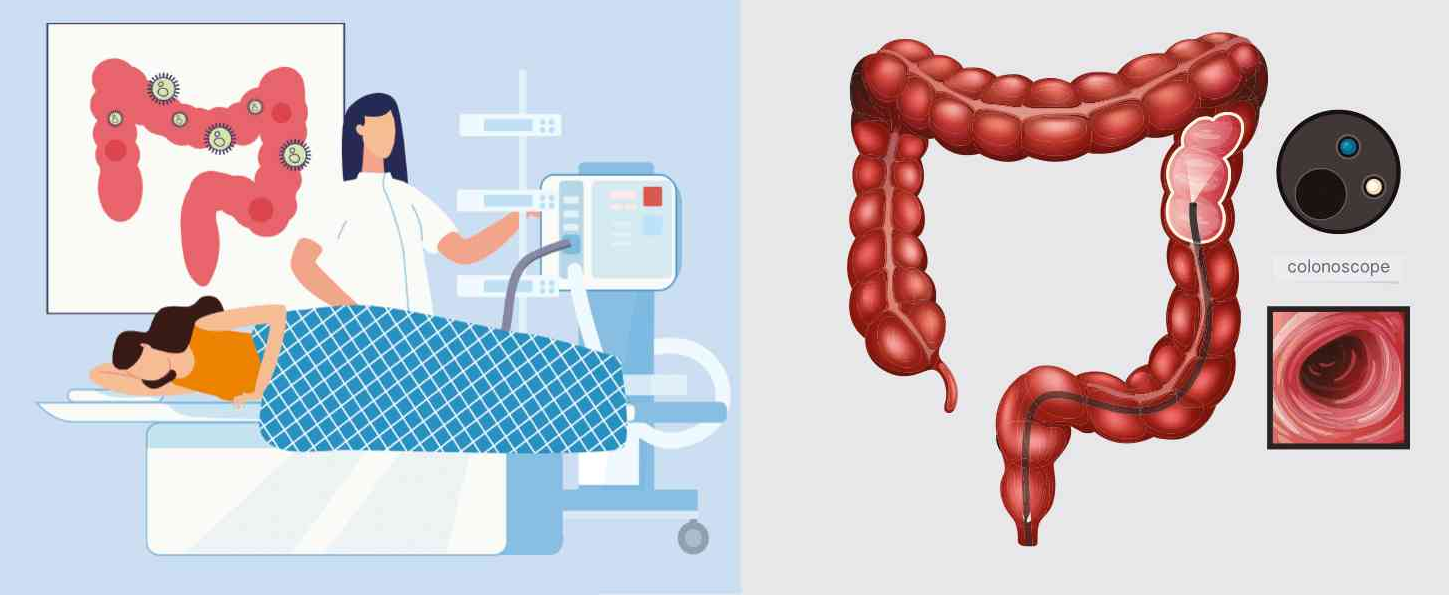
A rectal exam may be conducted to diagnose certain diseases. Certain types of cancers may be diagnosed by performing an endoscopy in the rectum. An endoscopy is a procedure where a doctor uses an endoscope- a small, flexible tube with a camera and light- to examine areas inside the body. Body temperature may also be obtained from the rectal area. In the case of infants and babies, this is generally the most accurate method for determining actual body temperature.
Based on diagnosis, your doctor will treat the condition or illness.